2016
Chapter 7
COMMUNICABLE DISEASE CONTROL
A local health director must be thoroughly familiar with the history of infectious disease outbreaks in the community and must exercise active (require formal periodic reports) and passive (accept voluntary reports) surveillance from physicians, laboratories and hospitals. The dwereirector needs to be aware of the community's demographics to prepare for the diseases most likely to strike. The director should know the community's level of "herd immunity" for the major infectious diseases. The department must have a plan to control epidemics. While communicable diseases may be so well-controlled that months pass without incidents, epidemics are marvelous opportunities to pull the staff together as a team and demonstrate the effectiveness of public health programs to the community. This has become even more important with all the anxiety over potential pandemics such as Avian Swine derived Influenza, The H1N1 “epidemics” of 2010 and 2012, each new Avian Flu serotype coming out of China and a continued concern for bioterrorism.
The director must translate national objectives into effective local programs of communicable disease control. In smaller jurisdictions it makes sense to combine disease surveillance, immunization, and infectious disease control (of all types) into a single program, supervised by a staff member trained in epidemiology. The focus of diseases to be controlled are discrete categories in the Healthy People 2020 recommendations; with three Objectives HIV, Immunization and Infectious diseases, and Sexually Transmitted diseases.
While they are discussed separately here, in practice such compartmentalization strains the resources of smaller agencies. Managing childhood infections as a program separate from adult infections, or treating community surveillance as a program distinct from both, is organizationally inefficient at the state or local level. Infection control requires the use of geographic epidemiology and analysis of disease rates by age, sex, race, culture and socio-economic levels. Epidemiologic skills are similar for different diseases, whether they happen to be insect borne, by respiratory routes, skin contact or sexually transmitted. Treatment for tuberculosis or Hansen's disease, immunization for measles or diphtheria and surveillance for Hepatitis-A and B, or regional diseases such as encephalitis, dengue and malaria are all part of a sound infectious disease program. When developing your goals and plans look at the data and recommendations available on both the CDC and WHO websites. The CDC has four separate websites;
Office of Public Health Preparedness and Response
National Center for Immunization and Respiratory Diseases (NCIRD)
National Center for Emerging and Zoonotic Infectious Diseases
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
Healthy People 2020 goals for immunization and infectious diseases are rooted in evidence-based clinical and community activities and services for the prevention and treatment of infectious diseases. Objectives new to Healthy People 2020 focus on technological advancements and ensuring that States, local public health departments, and nongovernmental organizations are strong partners in the Nation’s attempt to control the spread of infectious diseases. Objectives for 2020 reflect a more mobile society and the fact that diseases do not stop at geopolitical borders. Awareness of disease and completing prevention and treatment courses remain essential components for reducing infectious disease transmission
The infectious disease public health infrastructure, which carries out disease surveillance at the Federal, State, and local levels, is an essential tool in the fight against newly emerging and re-emerging infectious diseases. Other important defenses against infectious diseases include:
CDC National Public Health Performance Standards Program (NPHPSP) NPHPSP is a National Partnership initiative that has developed National Public Health Performance Standards for state and local public health systems and for public health governing bodies. This site provides information on the NPHPSP, the National Partners, and the resources available to support performance assessment and systems improvement. NPHPSP and National Partner staffs offer technical assistance, performance assessment analysis reports, and systems planning services to users of our assessment instruments. NPHPSP performance assessments should provide system participants with an understanding of the gaps between their current performance and the optimal level of performance described by the standards. System partners can then determine where the largest or most crucial gaps in performance are; these are the areas on which the action plan should focus.
It has become increasingly clear during the last few years that the database for infectious disease control and reporting is a priority. This is accomplished through the public health informatics and technology program office whose mission is to support health and public health practices by encouraging better management and use of information and knowledge. This has been developed the public health information network (PHIN), which promoting the use of standards and defining functional and technical requirements. The PHIN strives to improve public health by enhancing research and practice through best practices related to efficient, effective, and interoperable public health information systems.
The single most effective barrier to any communicable disease in the population is widespread immunity to that disease. Routine immunization of children against a host of potentially devastating illnesses is an inexpensive and effective way to build that barrier. In the U.S., immunization is required by law at entry into school in all 50 states and the District of Columbia.
Further, the 2020 objectives identify the Emerging Issues in Immunization and Infectious Diseases for the coming decade, the United States will continue to face new and emerging issues in the area of immunization and infectious diseases. The public health infrastructure must be capable of responding to emerging threats. State-of-the-art technology and highly skilled professionals need to be in place to provide rapid response to the threat of epidemics. A coordinated strategy is necessary to understand, detect, control, and prevent infectious diseases. Below are some specific emerging issues.
Providing culturally appropriate preventive health care is an immediate responsibility that will grow over the decade. As the demographics of the population continue to shift, public health and health care systems will need to expand their capacity to protect the growing needs of a diverse and aging population.
Following the Terrorist attack on New York in 2001 the federal government, through the CDC provided millions of dollars to provide epidemiologists to most local health departments to ensure better surveillance for both infectious and chemical agents. The CDC also proved funds to enhance electronic surveillance and reporting systems to provide rapid transmission of potential hazards to the CDC and national homeland security centers.
Following legislation in 2003 the State Department of Health, as well as other state agencies, has been required to complete and update a strategic plan. This can be viewed to look at current long range objectives by health objectives. Toward the end of each section you will find a description of the objectives and measurements accompanying them (note that it needs updating from 2011.).
Local objectives
In a typical health department the long-range local goals will be similar to the state objectives. The short-term goal is based on the actual resources available for the next year. Therefore, a local short-term goal for a model LHD was:
No additional local objectives were made because there was no way to measure them. When the local objectives were set for the 300,000 people in the County the incidence of preventable childhood infections was too small to measure change in any useful way, compared to the whole state. Such measurements are only useful with much larger populations. For this reason, more appropriate and measurable performance objectives were chosen
The second objective was used to prepare a budget for immunizing children that required a total of five DTP shots, three polio doses and one dose each of measles, mumps, and rubella vaccines before school entry. Birth certificates which describe how many children are born, and where, were used to set a second objective. Since this objective was stated more immunogens have been introduced which require more staff and better measurements of function.
To encourage parents to bring their children in for immunization and ensure the department met its goals pre-and post-natal education programs emphasized the need to vaccinate children, while visits by nurses and social workers to child & infant day care centers were used to reinforce the need for immunization. Records from clinic sessions in previous years show how much vaccine was used, and surveys of schools and day care centers measure the vaccination compliance level at time of entrance to school.
Currently with the expansion available vaccines and the complexity of the dosing, it is necessary for local and state agencies to have electronic records to evaluate the effectiveness of their programs. Until all physicians’ offices also have such systems the surveillance will always by tentative, although federal law has mandated that such record systems be installed by 2014! While this was technically possible the funding was insufficient for small primary-care practices although the Affordable Care Act was expected to provide funds to small practices to develop electronic data systems. The problem still exists that no single nationwide template has been developed and many of the plan systems have no capability to interchange data with each other, such as sending data to and from the local practice to the local hospital and back.
Immunization tracking
Data systems should track a child's immunization by type, number, and interval to the next dose of vaccine. With appropriate tracking software, described in the section on data systems, computer generated reminders can be sent to parents prior to the child's next clinic appointment. If the child does not come in, the system sends a reminder to a nurse or immunization aide to make a home visit to check on the child and family. Good software ensures adaptability, allowing the system to extract data from birth records, and remind parents that their new baby needs to be immunized, by either the family physician or the health department. A data system may be modified to account for local behavior, provide information in different languages, send out interpreters, and provide pamphlets or other visual advice to persons who may be illiterate. One advantage of performing your own programming is the ability to build in locally useful data, such as census tracts, language needs, and educational levels. The program can generate messages most suitable to each particular neighborhood. Review the CDC’s updates on immunization information systems webpages which were last updated in October 2015, including functional standards.
A local department's immunization system should be linked to state and federal immunization programs. This allows remote evaluation of the program, without the need to produce additional data. The system should provide information about the number of individual children previously fully immunized, the number starting immunization, the number completing immunization, the number with delayed completion and actions planned to complete the required immunizations. Data on individual doses used should be passed to the department's supply system automatically to ensure that sufficient vaccine is always on hand. A small inventory, keeping only necessary stock, prevents vaccine from becoming outdated and saves money. In many states this was accomplished by 2009.
The data system keeps the local immunization manager abreast of the program's effectiveness (number of persons at risk who are completely immunized) and efficiency (the number completing immunization with minimal or no recalls, by census tracts). The health director may not appear to need such an elaborate data system in a small community, but where there is more than one clinic at one site a month, such a system has an enormous effect on the department's operations where records are completed by hand, the same data is often gathered in different formats and provides a major opportunity for errors in recording. It also prevents an accurate count of doses used, and persons immunized, unless the records are complex and redundant. Also, as adult immunization status becomes more important, with immunizations for hepatitis b, pneumonia, tetanus, and other diseases the data systems can easily be extended to include everyone in the community, if desired. A review of lessons learned about immunization tracking can be found at the Robert Wood Johnson Foundation (Richmond City Health Dept. was one of the originals 12 recipients of AKC grants, the Co-Investigator was Dr. Buttery) for the all kids count and other programs for immunization development and enhancement
Sexually Transmitted Diseases
Public health officials have known how to control STDs for at least 50 years, but eradication remains difficult. In the 1940s, the treatment for tertiary syphilis was by infection with malaria, in the hope that the high fever of a malarial crisis would kill the temperature sensitive syphilis bacterium but not the patient (host.) This treatment was abandoned in the latter part of that decade when penicillin was found to be effective against all forms of syphilis. It is unfortunate that HIV infection has not been treated as just another serious STD, and less time wasted in political battles. When developing plans to control HIV, local health department staff should remember lessons learned from controlling syphilis and tuberculosis infection, which included public education, screening for disease, contact tracing, compilation of confidential disease registers, development of State and regional objectives.
State objectives for STDs tend to follow the 2020 Objectives in setting outcomes by disease. The 2020 plan now has 32 objectives, which while fine at the national level become overwhelming at the local and even at the state level. For STDs and the HP 2020 goals and objectives had been considerably changed, from those seen in the HP 2000 and HP 2010 publications:
STDs refer to more than 25 infectious organisms that are transmitted primarily through sexual activity. STD prevention is an essential primary care strategy for improving reproductive health. Despite their burdens, costs, and complications, and the fact that they are largely preventable, STDs remain a significant public health problem in the United States. This problem is largely unrecognized by the public, policymakers, and health care professionals. STDs cause many harmful, often irreversible, and costly clinical complications, such as:
Local objectives.
Many local health departments start their plans with the most current Healthy People Objectives, but integrate them into the community's economy, health care and human service systems. Local advisory boards can help to set reasonable goals and objectives in relation to the community's problems and resources and with health departments reaching and exceeding those objectives, an annual review of plans is essential, while complete revision is advisable at least every four years. Each revision of the planning process (community health assessment) should try to improve its data, as well as the infrastructure necessary to deliver and measure services, and better acceptance of programs. One advantage of public health planning, over that of mental health, is that measurement of changes in physical health outcome is usually easier to define. Many mental health results are measured as behavioral changes. It is simpler to measure a blood sugar, blood pressure, or to culture a bacterium than to measure behavioral changes. Diabetics can be tracked with blood tests while changes of behavior by substance abusers may be difficult to validate.
When setting objectives for STDs the health director needs to take special care to examine the local organization, delivery, and program accountability. STDs although diagnosed by laboratory tests have a large behavioral health component. Different STDs may have different behaviors associated with them. Exposure to one STD is often accompanied by infection with a second. Objectives to decrease the incidence of STDs should include behavioral measurements. For instance, gonorrhea is usually associated with heterosexuality, except that rectal gonorrhea is mainly a homosexual disease. Objectives for gonorrhea control should include processes to test patients for HIV and Hepatitis-B infection as well as Chlamydia and syphilis. Objectives for counseling and contact tracing may require cooperation with mental health professionals as well as infectious disease experts to define all the objectives needed for community-wide control of STDs. Many public health programs are only successful when other agencies are included in both goal setting and program service.
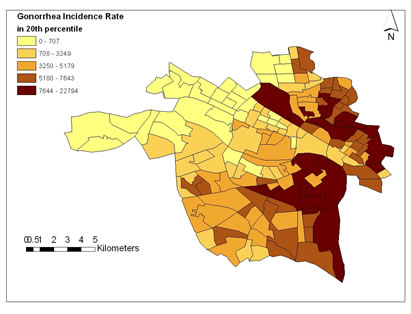
Setting objectives and obtaining resources to reach the objectives is often more difficult outside urban centers where many legislators think of STDs as something you get for breaking community mores, and that catching the disease is a “well deserved” lesson. It may be difficult to get a city council to consider the need for additional funding of STD programs. If local health departments focus on low-income areas and on young people from puberty through 20 years of age, they find gonorrhea in 4,000-5,000/100,000 persons at risk rather than in the 200-300/100,000 range expected for the total population. Without epidemiologic studies to identify high-risk groups, and efforts to contact them and get their trust, the health director has little to discuss with city and county officials other than generalities. Personal testimony about what is actually going on in their community has much greater impact.
For example, the above map can have great impact on a city council which shows very clearly where resources should be placed to combat STDs in this city.
One local plan in a city-county health district of 300,000 people was developed after data showed that syphilis incidence increased from 227 to 271 cases, while gonorrhea decreased from 1278 to 1019 cases. Additionally, an outbreak of hepatitis-A started from an index case as a sexually transmitted infection. These data led to an objective to:
Increase the number of STD patients seen from 1,850 to 2,200 and to continue development of the AIDS programs
To do this, the department needed an additional STD investigator, one public health nurse, two community service aides, and three clerks.
In many local health departments immunization, tuberculosis, and STD programs are part of a combined infection control program. In the local department described in the preceding paragraph immunization accounted for 60% of the infection control program budget (including vaccine cost), tuberculosis 10%, and STDs 30%. The whole cost of the program was $226,877 or 5% of the department's total budget.
Communicating with the public.
The success of public health programs in controlling communicable disease makes it difficult to fund their continuation. Without community-wide education the general public, and government officials alike, are all too likely to assume a disease has been eradicated when it is only out of sight. Dramatic outbreaks of new Infections like SARS or Legionnaire's disease, raise people's consciousness about these particular threats, but do not foster an overall understanding of the nature of infectious diseases and the need for continuing measures to control them.
Control of infectious diseases is the broadest possible public health activity. It includes nearly every other activity we undertake--childhood immunization, school health, clinical services, detection, screening, sanitation, insect spraying, water and wastewater management, sex education, food protection, etc. This breadth makes the topic difficult to grasp, as many of the results can only be expressed clearly with statistics. Public education, then, becomes a vital step in disease control. When the public understands how a disease works, how it is transmitted and what conditions promote its spread, they understand a rate reduction by 2 cases per 100,000, not as two individuals somehow receiving special treatment, but as an indicator of disease control that prevents them from being stricken themselves. If such understanding is widespread in the community, the health department will have little trouble getting support for its programs. More importantly, the citizens are actively involved in creating a healthier community.
Health education takes many forms: staff teams can be developed to talk about the nature of communicable diseases, in formal teaching sessions in schools and community agencies and as invited speakers at club meetings. The mechanics of the reservoir and vectors of, and host responses to, particular diseases can make excellent stories for the press; it may even be possible to produce a weekly column on these topics for a local newspaper or a short taped program for radio or TV. Whenever staffers deal with community members directly in immunization clinics, home visits or elsewhere, they should be encouraged to explain what they are doing and why it is important. Vector control, animal control, and sanitarian staff have hands-on knowledge of infection possibilities, and direct experience is more meaningful than statistics for all of us.
Because no one agency or group working in isolation can be effective, disease control requires some effort and attention from all of us. This can be made clear by describing, in detail, the accomplishments of everyone involved in communicable disease control including the private practicing physicians and hospital staff members who help prevent epidemics, the voluntary agencies that help make immunization programs work and the sixth grade class that spent a Saturday cleaning trash from a stream. The health department that attempts to take all the credit for good health is probably in trouble. The one that shares the spotlight and praises others will tend to get the cooperation it needs.
In one community the local health department, school system, and private pediatricians worked closely together to raise immunization levels enough to produce herd immunity and prevent further disease when a measles outbreak occurred. After five years without a single reported case of the disease, the community was struck by four cases, reported on a single Monday morning, all identified by older pediatricians who knew what 'Koplik's' spots were. Because the health department knew the immunization efforts had produced a high immunity level in the school system, it expected the outbreak to be contained. With the close cooperation of the community, built up over the years, the department staff contacted the school principals and parents for permission to draw blood from all students at the two schools initially reporting measles cases. The permission was given within 24 hours. Within 48 hours, blood was drawn from more than 75% (1400) of the students at the two schools. Blood was drawn again three weeks later, by which time more than 130 definitive cases of measles had occurred. Antibodies from the blood drawn before the infection became widespread showed measurable measles titers for more than 97% of the students sampled, confirming the accuracy of the immunization records in the schools. Out of a school population of almost 60,000, the disease was confined to 350 students. The community was given an excellent example of shoe leather epidemiology by a department seen as doing everything possible, by both the general population and the medical community. An open discussion with the media, of all the department's actions during the epidemic, did much to maintain its credibility. Don’t forget the teaching opportunities of the department’s web site with linkages to the CDC.
Recommended Reading: